 The procedure known as Knee Replacement requires an orthopaedic surgeon to precisely measure and remove portions of worn cartilage and bone before resurfacing the joint. Once the bone is resurfaced and re-shaped a prosthesis is implanted to facilitate fluid movement in the knee joint on recovery from the operation.
Partial and Total Knee Replacement There is what is called the uni-compartmental or partial Knee Replacement, (hemi-arthroplasty) or the Total Knee Replacement, (arthroplasty). These procedures are optional when patients have arthritis or injuries that severely impact their ability to execute simple everyday activities like walking around the house. Generally, other treatments such as medications, walking aids, physiotherapy and exercises are undertaken before surgery is recommended. The types of diseases that can lead to Knee Replacement are:
Plastic components, (Polyethylene) The plastics used are a specialised form of polyethylene called ultra-high molecular-weight polyethylene, (UHMWPE). A common example of the materials used in a Total Knee Replacement that include polyethylene are; the tibial component is a metal stem topped by a flat plate; then there’s the polyethylene cushion or bearing surface positioned between it and; the contoured metal surface of the femoral component. Lastly, there is the possibility that a dome-shaped polyethylene component can be used as a cushion for the patella. Though there can be multiple variants of the materials used for each component. Metals Materials used Variants of the types of metal prosthesis materials used are:
0 Comments
 How common is knee arthroscopy? An Australian Commission on Safety and Quality in Health Care study shows that in 2012-13, the number of admissions for knee arthroscopy in Australia was 33,682. Of that number, those who were 55yrs old or over counted for 560 admissions per 100,000 people1. Knee arthroscopy in Australia is an important procedure for both diagnostic and therapeutic purposes. Knee arthroscopy has become the gold standard in the diagnosis and management of menisci, ligament and articular cartilage injuries. More recently, knee arthroscopy has also produced encouraging results in the treatment and management of osteoarthritis. Although this success is sometimes due to the treatment of parallel conditions of the knee which aggravate osteoarthritis, the affect delays the onset and severity of its symptoms. Knee Arthroscopy can prevent the need for more invasive surgeries: Another study conducted between 2000 and 2008 shows within the first 24 months of having primary knee arthroscopy there was a decline in the number of people needing a follow-up total knee replacement. This decline is in opposition to other, more recent knee surgery trends, such as; the steady increase, by approximately 500 to a 1000 admissions per year, for total knee replacements between 2008-09 and 2013-143. This suggests although doctors believe more knee replacements are necessary, some who have knee arthroscopy are managing to postpone if not cancel replacement. Osteoarthritis sufferers benefit too: The first statistic shows the increasing effectiveness of knee arthroscopy in Australia, in treating knee injury or disease. The decline also occurred across all age groups, so applies to those older age groups more likely to suffer from degenerative disease. This is significant because degenerative diseases are harder to treat and the single most common reason for patients over 55yrs old to undergo knee replacement surgery. How common is osteoarthritis? To get some perspective on just how common osteoarthritis is, there are approximately 1.3 million people in Australia who experience the condition. But, because it is a gradual degenerative disease, there can be a long time between the first sign of any symptoms, and the need to have arthroscopy or more invasive forms of surgery. Although osteoarthritis is an older person’s disease, those in their 20’s and 30’s can also experience the condition. Of all hospital admissions for elective surgery in 2012-13, 1 in 7 were for osteoarthritis. Although any joint in the body can become affected by osteoarthritis, the weight bearing joints such as the knee and hips are the most commonly operated on. These are then followed by the fingers, hands and spine. Notes:
 Gary’s Right Knee: Gary is yet to have any form of knee surgery and last saw Dr Coffey in December of 2015. He is a prison officer who experiences a number of pains around his lower back, upper right leg and right knee. This has been an ongoing condition for over a year. Gary still gets numbness and tingling in his thigh, pain in his calf and a pinching in his hamstrings. These pains cause him to toss and turn at night making it difficult to get back to sleep. After conversation, Dr Coffey isolates the thigh pain to Gary’s pre-existing ‘meralgia paresthetica’, though thinks the pains lower in the leg could be secondary symptoms of Gary’s knee issues. When asked if Gary can walk without pain he demonstrates by lifting himself out of his chair and limps before he regains his natural stride. Apparently he used to enjoy walking for recreation and to keep his weight in check but says because of the discomfort he no longer walks as often. 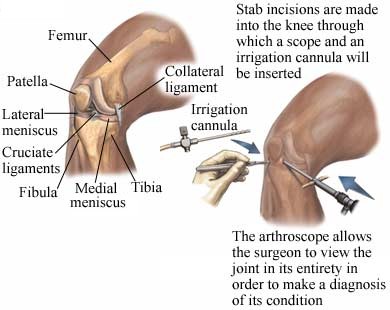 Torn Meniscus:
After a physical examination Dr Coffey reviews the X-Ray and MRI Scan, to explain Gary’s knee cartilage has a slight tear. The position of the torn piece of cartilage means the meniscus isn’t fully functional. There is also a degree of cartilage thinning but the torn piece of cartilage catching on the roll of the knee is causing the majority of his pain. There are also degenerative changes in Gary’s back which could be causing some of the pain. But due to sciatica being unpredictable it is harder to determine. Dr Coffey then talks about Gary’s treatment. Arthroscopy: Gary’s torn cartilage makes him a candidate for an arthroscopy. This is a minimally invasive form of intervention where a thin headed arthroscope, (telescope), is inserted into a small incision on the knee. These small incisions are the keyholes of keyhole surgery. The arthroscope is then moved into the site of the source of pain within the joint. In Gary’s case the telescope would locate the torn piece of cartilage and efforts would be made to trim the loose cartilage away from the meniscus plate as a whole. The option of an arthroscopy means Gary could be in and out of hospital in a single day. Post-op Gary can walk on his knee as he feels comfortable. As for returning to work he can go back in a couple of weeks. This delay is only due to the potential physical nature of his work, (being a prison warden). Otherwise he could sit in front of his computer screen the moment he got home. The recovery process is to be taken steadily, not rushed or avoided. And when Gary does go back to work he’d need to take on lighter duties until his full strength returned. Time will tell: Before Gary leaves he asks Dr Coffey; ‘If he should have an arthroscopy now or wait?’, and; ‘if walking without having surgery would just tear his meniscus and make surgery more inevitable?’ Dr Coffey said the answer to both his questions was up to his pain: ‘If your knee is painful enough then surgery is worth thinking about, because the tear in the meniscus is not going to go away. As for activity tearing the meniscus; it’s always a possibility you could increase the damage, but not walking to avoid it happening was self-defeating.’ Dr Coffey then recommends that the wait and see approach was still open to Gary, but that any worsening of his pain would mean an arthroscopy was necessary. |
ArchivesCategories |
 RSS Feed
RSS Feed
